







Sedation practice for endoscopy varies widely in the United States. One model is to use anesthesia specialists to administer propofol for complex endoscopic procedures, such
EMR
Are Anesthesia Specialists Necessary for Complex Colorectal Endoscopic Mucosal Resections?
Are Anesthesia Specialists Necessary for Complex Colorectal Endoscopic Mucosal Resections?
Colon Polyps Extending Across an Anastomosis Can Be Effectively Removed by Endoscopic Mucosal Resection
Colon Polyps Extending Across an Anastomosis Can Be Effectively Removed by Endoscopic Mucosal Resection
Among 2629 large nonpedunculated colorectal polyps in 2350 patients, 10 were classified as anastomotic and had a median lesion size of 35 mm. All lesions
Post-EMR Adenoma Recurrences Are Effectively Treated Endoscopically
Post-EMR Adenoma Recurrences Are Effectively Treated Endoscopically
About 15% of large (≥20 mm) nonpedunculated colorectal polyps (LNPCPs) removed by piecemeal endoscopic mucosal resection (EMR) have evidence of recurrence at the first endoscopic
European Society of Gastrointestinal Endoscopy Issues Comprehensive Curriculum for Endoscopic Mucosal Resection in the Colon
European Society of Gastrointestinal Endoscopy Issues Comprehensive Curriculum for Endoscopic Mucosal Resection in the Colon
Those performing endoscopic mucosal resection (EMR) in the colorectum should be aware of this remarkably comprehensive document from the European Society of Gastrointestinal Endoscopy that
Combined EMR and Full-Thickness Resection for Large Nonlifting Colorectal Adenomas
Combined EMR and Full-Thickness Resection for Large Nonlifting Colorectal Adenomas
Endoscopic submucosal dissection (ESD) is an option for scarred, large colorectal adenomas that do not lift well and/or contain a suspicious area of an advanced
Uncontrolled Description of X-Tack Efficacy for Colonic EMR Defects
Uncontrolled Description of X-Tack Efficacy for Colonic EMR Defects
X-Tack (Apollo Endosurgery, Austin, Texas) is a through-the-scope suturing device that can be an alternative to through-the-scope clips. No controlled trial of X-Tack versus clips
Cold Snare Resection, at Least Cold EMR, Looks Good for 10- to 19-mm Polyps, Including Adenomas
Cold Snare Resection, at Least Cold EMR, Looks Good for 10- to 19-mm Polyps, Including Adenomas
Cold snare polypectomy is the accepted treatment of choice for all colorectal polyps smaller than 10 mm and with no suggestion of cancer on endoscopic
Intravenous Acetaminophen Said To Distinguish Benign Postcolorectal EMR Pain From Pain Potentially Reflecting Complications
Intravenous Acetaminophen Said To Distinguish Benign Postcolorectal EMR Pain From Pain Potentially Reflecting Complications
In an observational study of colorectal EMR, 67 of 336 patients (19.9%) experienced postprocedural pain. All EMRs were performed with electrocautery and adrenaline injection. Pain
Should a Biopsy of Normal-Appearing EMR Scars Be Performed at Follow-up?
Should a Biopsy of Normal-Appearing EMR Scars Be Performed at Follow-up?
Traditionally, even if careful inspection of an EMR scar at follow-up shows no residual polyp, a biopsy should still be performed to rule out histologic
Male Gender and Hot Avulsion Are Associated With Recurrence After Colorectal Endoscopic Mucosal Resection
Male Gender and Hot Avulsion Are Associated With Recurrence After Colorectal Endoscopic Mucosal Resection
Endoscopic mucosal resection (EMR) is the cornerstone of the treatment of large (≥20 mm) nonpedunculated colorectal lesions. This study from a Canadian expert center examined
Snare Tip Soft Coagulation Reduced Recurrence After EMR in Routine Practice
Snare Tip Soft Coagulation Reduced Recurrence After EMR in Routine Practice
Thermal treatment of endoscopic mucosal resection (EMR) margin defects after complete resection of large (≥20 mm) nonpedunculated colorectal polyps has reduced the recurrence rate at
Study Shows Margin Treatment Was Good but Not Perfect for Colorectal Laterally Spreading Lesions 40 mm or Larger
Study Shows Margin Treatment Was Good but Not Perfect for Colorectal Laterally Spreading Lesions 40 mm or Larger
Thermal treatment of the margin after piecemeal endoscopic mucosal resection (EMR) of laterally spreading lesions (LSLs) ≥20 mm is now considered standard of care because
Endoscopic Submucosal Dissection Plus Radiofrequency Ablation Exhibits High Eradication Rates in Patients With Barrett’s Esophagus
Endoscopic Submucosal Dissection Plus Radiofrequency Ablation Exhibits High Eradication Rates in Patients With Barrett’s Esophagus
Current strategies for the endoscopic treatment of Barrett’s esophagus (BE) focus on resection of nodular lesions within BE and then the ablation of the flat
Impact of Preresection Biopsy on Subsequent Endoscopic Mucosal Resection
Impact of Preresection Biopsy on Subsequent Endoscopic Mucosal Resection
We often hear that physician-identified large nonpedunculated colorectal polyps (LNPCPs) that warrant referral to an advanced endoscopist for endoscopic mucosal resection (EMR) or endoscopic submucosal
Tip-in EMR Compared With ESD for 20- to 30-mm Nonpedunculated Colorectal Neoplasms
Tip-in EMR Compared With ESD for 20- to 30-mm Nonpedunculated Colorectal Neoplasms
Tip-in endoscopic mucosal resection (EMR) involves submucosal injection, followed by an incision on the proximal side of the injection mound using a snare tip with
Hybrid Argon Plasma Coagulation Endorsed to Reduce Recurrence Rate After Colorectal EMR
Hybrid Argon Plasma Coagulation Endorsed to Reduce Recurrence Rate After Colorectal EMR
Thermal coagulation of the normal-appearing margin using snare tip soft coagulation (STSC) treatment after endoscopic mucosal resection (EMR) has been shown to reduce recurrence rates
Pilot Study Finds Submucosal Thickness Is Greater With Colorectal EMR Than ESD
Pilot Study Finds Submucosal Thickness Is Greater With Colorectal EMR Than ESD
Discussions of colorectal endoscopic mucosal resection (EMR) versus endoscopic submucosal dissection (ESD) usually focus on en bloc resection and recurrence rates. Little is known about
ORISE Associated With Submucosal Fullness and Distortion at Follow-Up EMR
ORISE Associated With Submucosal Fullness and Distortion at Follow-Up EMR
ORISE (Boston Scientific, Marlborough, Mass, USA) is a viscous gel for submucosal injection. When ORISE is used for endoscopic mucosal resection (EMR) or endoscopic submucosal
Is Cold Snare Piecemeal EMR Adequate in Treating Duodenal Adenomas?
Is Cold Snare Piecemeal EMR Adequate in Treating Duodenal Adenomas?
Traditionally, nonampullary small-bowel adenomas ≥10 mm in diameter are resected utilizing cautery. Unfortunately, since the small bowel is thin-walled and highly vascular, adverse events are
Clip Closure Did Not Reduce Delayed Hemorrhage After Resection of Large Sessile Serrated Lesions Using Electrocautery, Even From the Proximal Colon
Clip Closure Did Not Reduce Delayed Hemorrhage After Resection of Large Sessile Serrated Lesions Using Electrocautery, Even From the Proximal Colon
Recent large randomized controlled trials have demonstrated that clip closure reduces the risk of delayed hemorrhage after endoscopic mucosal resection (EMR) using electrocautery if the
Endoscopic Submucosal Dissection Use Changes Histologic Diagnosis in More Than Half of All Patients With Visible Barrett’s Esophagus Neoplasia
Endoscopic Submucosal Dissection Use Changes Histologic Diagnosis in More Than Half of All Patients With Visible Barrett’s Esophagus Neoplasia
Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) have emerged as important treatment techniques for patients with visible lesions in Barrett’s esophagus (BE). Whereas
Epinephrine Caused Increased Postprocedural Pain When Used for Colorectal EMR
Epinephrine Caused Increased Postprocedural Pain When Used for Colorectal EMR
Including epinephrine in the submucosal injectate for endoscopic mucosal resection (EMR) varies among endoscopists – some endoscopists prefer epinephrine, whereas others do not. Of those
Should We Mark the Margins Before EMR?
Should We Mark the Margins Before EMR?
One approach sometimes used in endoscopic mucosal resection (EMR) to improve complete resection is to use cautery to mark the normal tissue at the margins
Randomized Controlled Trial Confirms Clipping Is Effective in Prevention of Right-Sided Colon Bleeding After EMR With Electrocautery
Randomized Controlled Trial Confirms Clipping Is Effective in Prevention of Right-Sided Colon Bleeding After EMR With Electrocautery
Previous randomized controlled trials (RCTs) have indicated that prophylactic clip closure is effective in preventing delayed hemorrhage after EMR of colonic lesions that are ≥20
Laterally Spreading Lesions With Focus of T1 Cancer Treated by Hybrid EMR and EFTR
Laterally Spreading Lesions With Focus of T1 Cancer Treated by Hybrid EMR and EFTR
Patients with laterally spreading lesions and endoscopic evidence of T1 cancer (usually of morphologic change combined with NBI International Colorectal Endoscopic classification 3 or Kudo
Cap-Assisted Endoscopic Mucosal Resection Effective for Flat and Fibrotic Colorectal Polyps
Cap-Assisted Endoscopic Mucosal Resection Effective for Flat and Fibrotic Colorectal Polyps
Everyone performing EMR in the colorectum encounters flat or fibrotic polyp tissue that resists standard snaring. In a multicenter European study, 70 nonlifting polyps with
Problems With Colorectal EMR Training for Some GI Fellows
Problems With Colorectal EMR Training for Some GI Fellows
In a 2019-2020 academic year survey of all 1730 GI fellows in the U.S. regarding endoscopic mucosal resection (EMR) training and knowledge, the response rate
Tattoos Claimed Unnecessary for Finding EMR Scars
Tattoos Claimed Unnecessary for Finding EMR Scars
Referring physicians sometimes tattoo large nonpedunculated lesions before referral, and resectionists sometimes tattoo the resection site for easy identification of the scar later. Neither practice
Multicenter International Study Confirms That Snare-Tip Soft Coagulation of EMR Margin Dramatically Lowers Recurrence Rate
Multicenter International Study Confirms That Snare-Tip Soft Coagulation of EMR Margin Dramatically Lowers Recurrence Rate
A previous randomized controlled trial showed that thermal ablation of a normal-appearing EMR margin after complete polyp resection reduced the recurrence rate from 21% to
Can We Decrease Lesion Recurrence After Duodenal Endoscopic Mucosal Resection?
Can We Decrease Lesion Recurrence After Duodenal Endoscopic Mucosal Resection?
Laterally spreading lesions (LSLs) of the duodenum are increasingly being diagnosed and treated endoscopically. Although endoscopic resection of the thin and vascular duodenal wall is
Predicting Complete Closure of EMR Sites
Predicting Complete Closure of EMR Sites
Clip closure of endoscopic mucosal resection (EMR) defects ≥20 mm located proximal to the splenic flexure and removed by electrocautery is associated with a reduction
Piece-meal EMR eines ausgedehnten lateral- spreading type Adenoms im Rektum
Piece-meal EMR eines ausgedehnten lateral- spreading type Adenoms im Rektum
Piece meal EMR eines ausgedehnten lateral- spreading type Adenoms im Rektum
When Is Clip Closure of EMR Defects Cost-Effective?
When Is Clip Closure of EMR Defects Cost-Effective?
Randomized controlled trials demonstrate that prophylactic clip closure of endoscopic mucosal resection (EMR) defects of large (≥20 mm) nonpedunculated colorectal lesions effectively prevents delayed hemorrhage.
Postcolorectal Endoscopic Mucosal Resection Follow-up Is Essential
Postcolorectal Endoscopic Mucosal Resection Follow-up Is Essential
There is a well-known risk of adenoma recurrence after piecemeal endoscopic mucosal resection (EMR). In a single-center study of 2411 nonpedunculated lesions ≥20 mm in

DEGEA Web Seminar – Innovative Resektionstechniken praxisnah erklärt (FTRD® & RESECT+)
DEGEA Web Seminar – Innovative Resektionstechniken praxisnah erklärt (FTRD® & RESECT+)
Web Seminar zu innovativen Resektionstechniken mit Einblicken und Tipps aus Sicht der Assistenz und Pflege. Das Web Seminar verbindet Theorie & Praxis zu den innovativen
Computerized Imaging of Vessels in EMR Defects Predicts Postprocedural Bleeding
Computerized Imaging of Vessels in EMR Defects Predicts Postprocedural Bleeding
Recent studies indicate that prophylactic clip closure of postendoscopic mucosal resection defects from colonic lesions >20 mm in size and proximal to the splenic flexure
Low Incidence of Colorectal Cancer After Endoscopic Dysplasia Resection in Patients With IBD
Low Incidence of Colorectal Cancer After Endoscopic Dysplasia Resection in Patients With IBD
Given the paucity of high-quality outcome data, the optimal management of polypoid and/or nonpolypoid colonic lesions in IBD is an ongoing debate. Guidelines recommend that
Prophylactic Clipping Ineffective for Polyps Less Than 20 mm in Size
Prophylactic Clipping Ineffective for Polyps Less Than 20 mm in Size
Analyses of randomized trials indicate that prophylactic clipping of EMR sites ≥20 mm in size in the proximal colon reduces the risk of delayed hemorrhage.
ESD Versus EMR for Resecting Esophageal Neoplasia
ESD Versus EMR for Resecting Esophageal Neoplasia
Endoscopic submucosal dissection (ESD) is an effective method of resecting larger superficial esophageal lesions en bloc; however, it is fraught with advanced training needs, longer
Microprocessor-Controlled Endo Cut Versus Forced Coagulation: No Difference in Delayed Hemorrhage
Microprocessor-Controlled Endo Cut Versus Forced Coagulation: No Difference in Delayed Hemorrhage
Douglas K. Rex, MD, FASGE, reviewing Pohl H, et al. Gastroenterology 2020 Mar 12. Previous uncontrolled studies indicated that forced-coagulation (FC) current (the blue pedal)

Sydney classification- assessment of deep mural injury after endoscopic mucosal resection.
Sydney classification- assessment of deep mural injury after endoscopic mucosal resection.
Classification presented by Burgess NG et al. based on retrospective evaluation, clinical observations and image analysis. It allows for the assessment of deep mural injury
Expanding Cold EMR to Large Laterally Spreading Lesions
Expanding Cold EMR to Large Laterally Spreading Lesions
Douglas K. Rex, MD, FASGE, reviewing Mangira D, et al. Gastrointest Endosc 2020 Jan 15. In 5 Australian academic hospitals, cold EMR was performed on
For Left-Sided Colon Lesions up to 25 mm and Right-Sided Colon Lesions up to 20 mm, Piecemeal EMR Is as Good as en Bloc Resection
For Left-Sided Colon Lesions up to 25 mm and Right-Sided Colon Lesions up to 20 mm, Piecemeal EMR Is as Good as en Bloc Resection
Douglas K. Rex, MD, FASGE reviewing Tate DJ, et al. Gastrointest Endosc 2019 Dec 27. Advanced endoscopists are often tempted to remove laterally spreading lesions
EMR eines Adenoms im C. transversum
EMR eines Adenoms im C. transversum
EMR eines Adenoms im C. transversum ECN 2018

Endoskopische Mukosaresektion eines Rektumadenoms
Endoskopische Mukosaresektion eines Rektumadenoms
Endoskopische Mukosaresektion eines Rektumadenoms ECN 2018

Underwater Koloskopie mit Polypektomie eines Rektumadenoms
Underwater Koloskopie mit Polypektomie eines Rektumadenoms

degea live – Pflege führt Regie – 21.03.18 – Teil 3: Multiple Polypen Hot & Cold Snare
degea live – Pflege führt Regie – 21.03.18 – Teil 3: Multiple Polypen Hot & Cold Snare
Teil 3 des degea Live-Streams vom 21.03.2018 – Multiple Polypen Hot & Cold Snare

degea live – Pflege führt Regie – 21.03.18 – Teil 2: EMR eines Colonpolypen
degea live – Pflege führt Regie – 21.03.18 – Teil 2: EMR eines Colonpolypen
Teil 2 des degea Live-Streams vom 21.03.2018 – EMR eines Colonpolypen

degea live – Pflege führt Regie – 21.03.18 – Teil 1: Vorsorgekoloskopie mit Kompressionstechniken
degea live – Pflege führt Regie – 21.03.18 – Teil 1: Vorsorgekoloskopie mit Kompressionstechniken
Teil 1 des degea Live-Streams vom 21.03.2018 – Vorsorgekoloskopie mit Kompressionstechniken

degea live – Pflege führt Regie – 21.03.18 – komplette Aufzeichnung
degea live – Pflege führt Regie – 21.03.18 – komplette Aufzeichnung
Dieser Live Stream vom 21.03.2018 betrachtet endoskopische Eingriffe durch die Brille der Assistenz und begleitenden Pflege. Dabei führt das Endoskopiefachpersonal Regie, unterstützt durch kompetente ärztliche
Kaltschlinge auf dem Vormarsch?
Kaltschlinge auf dem Vormarsch?
Die Kaltschlingen-Resektion hat sich bei sehr kleinen Polypen (bis 5 mm) als mindestens so sicher und potentiell mehr effizient als die Zangenentfernung oder teilweise auch

Kolonadenom / EMR
Kolonadenom / EMR
Gezeigt wird eine EMR bei Kolonadenom

ESD wohl nicht besser als EMR bei Barrett-Neoplasien
ESD wohl nicht besser als EMR bei Barrett-Neoplasien
Derzeit wird unter therapeutischen Endoskopikern viel über die beste Resektionsmethode bei frühen Karzinomen diskutiert, vor allem im oberen Gastrointestinaltrakt, während die Diskussion im Kolorektum aufgrund

Frühkarzinom des Ösophagus (Plattenepithel): Tipps und Trick bei der schwierigen ESD
Frühkarzinom des Ösophagus (Plattenepithel): Tipps und Trick bei der schwierigen ESD
Gezeigt werden Tipps und Tricks bei der ESD im Ösophagus

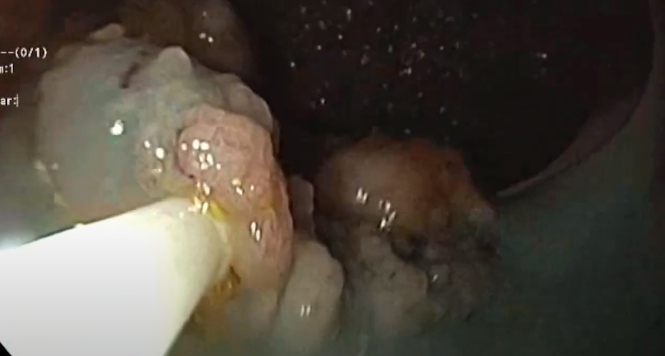
Post EMR – Arterielle Blutung
Post EMR – Arterielle Blutung
Gezeigt wird eine Nachblutung nach EMR im Ösophagus. Die Applikation von Hämoklipps gelingt nicht, daraufhin Anwendung einer Hot Biopsy Zange.
