Cap-Assisted Endoscopic Mucosal Resection Effective for Flat and Fibrotic Colorectal Polyps
Douglas K. Rex, MD, MASGE, reviewing Van der Voort VRH, et al. Endoscopy 2021 Sep 14.
Everyone performing EMR in the colorectum encounters flat or fibrotic polyp tissue that resists standard snaring.
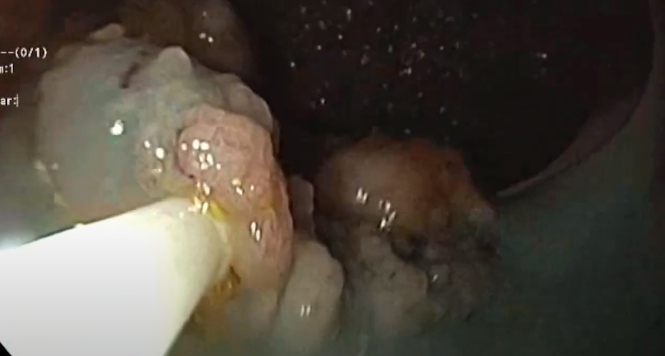
In a multicenter European study, 70 nonlifting polyps with a median size of 25 mm were treated with EMR using a cap on the end of the endoscope. The cap was positioned to extend about 4 mm beyond the end of the scope. Areas that resisted the cap method were treated with avulsion (n=8), ablation (n=6), or both avulsion and ablation (n=7).
The overall success of complete tissue removal was 97.1%, the overall recurrence rate at follow-up was 19%, and the rate of delayed bleeding was 8.8%. Complications included 1 transmural perforation (type 4 muscle injury) and 4 target signs (type 3 muscle injuries). All of the muscle injuries were closed with through-the-scope clips.

COMMENTI’ve used the cap technique for flat and fibrotic disease in colorectal EMR for more than a decade and in hundreds of cases, with only a single type 3 muscle injury. This lower risk of injury is almost certainly because I don’t put the cap out as far as that demonstrated in the photos from the current study. Cap-assisted EMR is more efficient than avulsion for removing flat and fibrotic disease if there is a larger surface area to remove, but avulsion is generally more effective than EMR because disease that resists removal with the cap technique will almost always submit to avulsion.
Available evidence suggests that ablation of visible polyp tissue should be abandoned in favor of the cap technique or avulsion, as ablation is associated with a higher recurrence rate. Colonoscopists are sometimes confused by the admonition to avoid ablation for visible residual tissue because ablation of the normal-appearing margin with snare-tip soft-coagulation thermal injury is advocated to reduce recurrence rates. However, ablation of visible residual polyp tissue is not recommended, whereas ablation of the normal-appearing margin after complete resection by snaring with or without avulsion is highly recommended. The two concepts regarding ablation must not be confused.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Van der Voort VRH, Moons LMG, de Graaf W, et al. Efficacy and safety of cap-assisted endoscopic mucosal resection for treatment of nonlifting colorectal polyps. Endoscopy 2021 Sep 14. (Epub ahead of print) (https://doi.org/10.1055/a-1559-2391)
Beiträge
Ähnliche Beiträge
Piece- meal EMR Rektum
Piece meal EMR eines ausgedehnten lateral- spreading type Adenoms im Rektum …

Sydney classification- assessment of deep mural injury after endoscopic mucosal resection.
Classification presented by Burgess NG et al. based on retrospective evaluation, clinical observations and image analysis. …
Polypektomie - Kaltabtragung
Die Kaltschlingen-Resektion hat sich bei sehr kleinen Polypen (bis 5 mm) als mindestens so sicher und …
