When Is Clip Closure of EMR Defects Cost-Effective?
Douglas K. Rex, MD, MASGE, reviewing Albéniz E, et al. Am J Gastroenterol 2020 Nov 3.
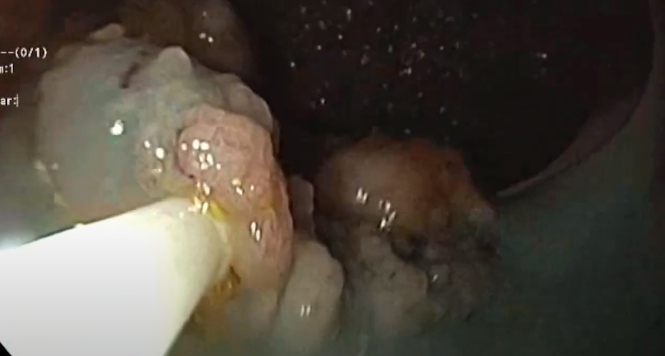
Randomized controlled trials demonstrate that prophylactic clip closure of endoscopic mucosal resection (EMR) defects of large (≥20 mm) nonpedunculated colorectal lesions effectively prevents delayed hemorrhage. In a meta-analysis, the benefits were present for lesions proximal to the splenic flexure. The practice is controversial, though, because of the high cost of clips.
In this study, the Spanish investigators who performed one of the randomized controlled trials performed a cost-effectiveness analysis to determine which lesions are cost-effective to clip. In the U.S., the accepted threshold for cost-effectiveness is an incremental cost-effectiveness ratio (ICER) of <$100,000 per quality-adjusted life-year. The analysis showed that if the delayed bleeding risk score was ≥7, according to the risk score model from the Spanish Endoscopy Society EMR Group (GSEED-RE2), the U.S. ICER was $87,796.
The GSEED-RE2 score ranges from 0 through 9, with 1 point for comorbidity or American Society of Anesthesiologists (ASA) physical status classification of III or IV, 2 points for lesion size ≥40 mm, and 3 points each for location proximal to the splenic flexure and antiplatelet or anticoagulant agents.
In the actual high-risk group (52% of the whole cohort), all of the patients had lesions proximal to the splenic flexure and were prescribed antiplatelets or anticoagulants, 99.2% had ASA III or IV or comorbidity, and 20.6% had a lesion size ≥40 mm.

COMMENTThis study suggests a set of criteria for when clip closure of EMR defects is cost-effective. Successful prevention of complications has additional appeal if it leads to greater willingness to do EMR rather than refer to surgery. Thus, simple effectiveness may be a better guide for when to clip close than is cost-effectiveness. If simple effectiveness is used as the guide, the target set of lesions for clip closure is nonpedunculated lesions ≥20 mm, proximal to the splenic flexure, and removed using electrocautery.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Albéniz E, Enguita-Germán M, Gimeno-García AZ, et al. The answer to „when to clip“ after colorectal endoscopic mucosal resection based on a cost-effectiveness analysis. Am J Gastroenterol 2020 Nov 3. (Epub ahead of print) (https://doi.org/10.14309/ajg.0000000000000943)
Beiträge
Ähnliche Beiträge
Piece- meal EMR Rektum
Piece meal EMR eines ausgedehnten lateral- spreading type Adenoms im Rektum …

Sydney classification- assessment of deep mural injury after endoscopic mucosal resection.
Classification presented by Burgess NG et al. based on retrospective evaluation, clinical observations and image analysis. …
Polypektomie - Kaltabtragung
Die Kaltschlingen-Resektion hat sich bei sehr kleinen Polypen (bis 5 mm) als mindestens so sicher und …
