
The Forrest Classification is now used as a tool to identify patients who are at an increased risk for bleeding, rebleeding and mortality
Upper GI tract
Upper GI tract
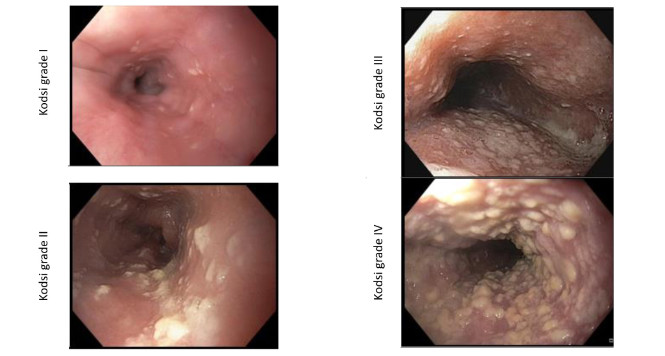
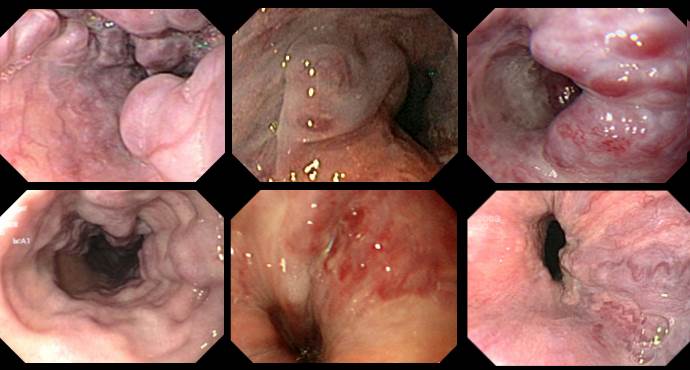
Kodsi classification of Candida esophagitis
Kodsi classification of Candida esophagitis
Candidiasis is the most frequent form of infectious esophagitis. The characteristic white plaques, which are difficult to rinse off, are found in approximately 4% of

Hiatus hernias and the Hill classification
Hiatus hernias and the Hill classification
To allow more precise assessment of the competence of the esophagogastric sphincter mechanism, Hill et al. presented a practical classification in 1996.

The CAES classification of anastomotic insufficiency in the esophagus
The CAES classification of anastomotic insufficiency in the esophagus
The Surgical Working Group on Endoscopy and Ultrasound (Chirurgische Arbeitsgemeinschaft für Endoskopie und Sonographie, CAES) has developed and validated a classification of anastomotic insufficiency in
Endoscopic removal of a buried bumper using the Flamingo system
Endoscopic removal of a buried bumper using the Flamingo system
A patient with an ingrown internal PEG retaining plate (buried bumper syndrome) on the anterior wall of the gastric body. Endoscopic removal of the device

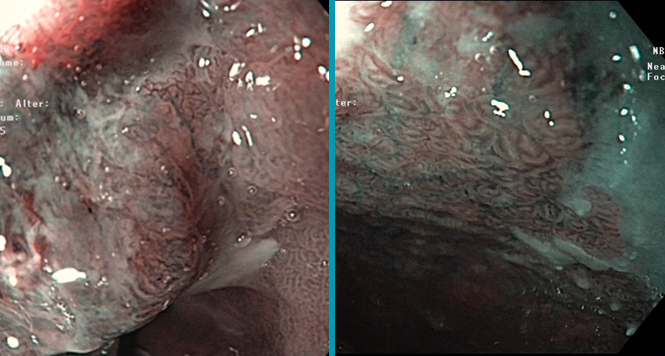
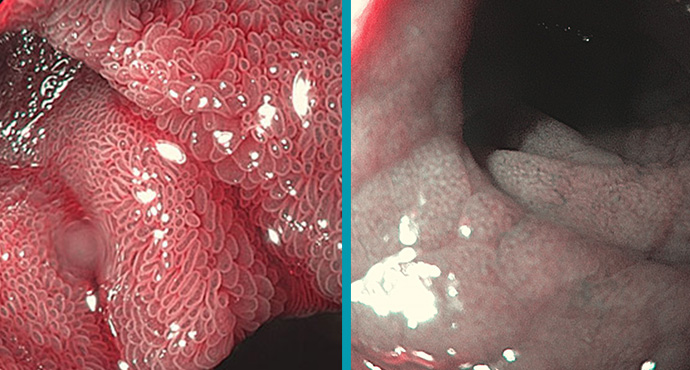
Stomach: Light Blue Crest Sign for Intestinal Metaplasia
Stomach: Light Blue Crest Sign for Intestinal Metaplasia
Gastric Intestinal Metaplasia is a risk factor of intestinal-type gastric cancer, but WLI was not adequate to detect IM of stomach. NBI system with and
BING Classification Early Barrett Neoplasia
BING Classification Early Barrett Neoplasia
Multimodal therapy for early Barrett’s neoplasias, has become established as the standard therapy and is set out in national and international guidelines. These dysplastic lesions

Achalasia: Chicago Classification
Achalasia: Chicago Classification
Achalasia is one of the differential diagnoses in patients with symptoms of dysphagia. High-resolution (HR) manometry is now regarded as the diagnostic gold standard for

Lars explains Anatomy – Gastric Bypass
Lars explains Anatomy – Gastric Bypass
Die Anzahl an durchgeführten Adipositas-OPs steigt weltweit. Für jeden Endoskopiker ist es wichtig die Anatomie nach einer Magen-Bypass-OP zu kennen um evtl. Komplikationen nach diesen

The bougie cap – a new method of treating stenoses in the gastrointestinal tract
The bougie cap – a new method of treating stenoses in the gastrointestinal tract
In the classic method, a stricture in the esophagus is dilated using a Savary bougie after advancement of a guide wire. The difficulty with this
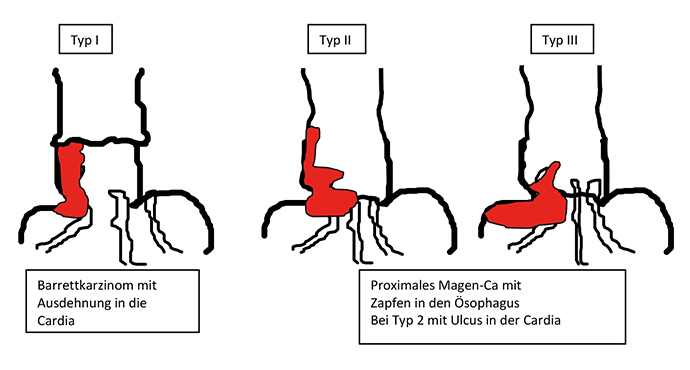
Esophagastric Junction Cancers (AEG)
Esophagastric Junction Cancers (AEG)
Tumors of the esophagogastric junction should be classified not only according to the TNM system with regards to tumor penetration (T stage), presence of lymph

Paris Classification: Early Barrett Cancers
Paris Classification: Early Barrett Cancers
In the following, examples for superficial/early Barrett lesions of the esophagus are shown. Here, flat and sessilelesions are predominant, pedunculated tumors are rare. Sessile tumor

Roux-en-Y anatomy after gastric resection
Roux-en-Y anatomy after gastric resection
This video illustrates the altered anatomy resulting after the type of gastric resection that is carried out for gastric carcinoma, for example. Bowel continuity is
Endoscopic full-thickness resection of a GIST using GERD-X
Endoscopic full-thickness resection of a GIST using GERD-X
A subepithelial tumor has been identified in the fundus. EUS shows that it is 2.5 × 3 cm in size, probably arising from the muscularis propria. No pathological

Billroth II anatomy after partial stomach resection
Billroth II anatomy after partial stomach resection
This video explains the altered anatomy that is encountered after a Billroth II operation. In a Billroth II resection, the lower part of the stomach
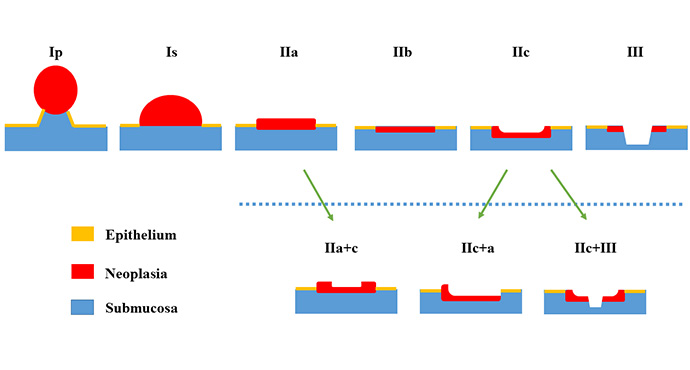
Paris Classification Early Cancer
Paris Classification Early Cancer
Endoscopic treatment for early carcinoma in the gastrointestinal tract has in the meantime become evidence-based and has been incorporated into national and international guidelines

Paris Classification: Early Squamous Cell Cancers Esophagus
Paris Classification: Early Squamous Cell Cancers Esophagus
Examples of superficial/early squamous cell lesions in the esophagus are presented below. In the esophagus, flat lesions are predominant in the early tumors, and polypoid

Paris Classification: Early Gastric Cancer
Paris Classification: Early Gastric Cancer
Examples of superficial/early gastric tumors are shown below. In the stomach, flat lesions are predominant, often as combined lesions with a central depression (IIa+c). Sessile

Gastric peroral endoscopic myotomy (G-POEM)
Gastric peroral endoscopic myotomy (G-POEM)
Hendrik Manner from Wiesbaden reports on a patient with a gastric emptying disorder who was treated with what is known as gastric peroral endoscopic myotomy

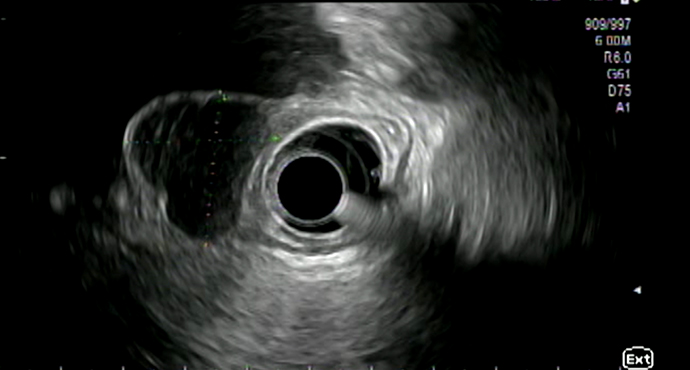
Distal hypoechoic submucosal tumor in the esophagus
Distal hypoechoic submucosal tumor in the esophagus
Submucosal lesions identified in the esophagus usually undergo further clarification using endoscopic ultrasonography (EUS). In this video, Thomas Rösch from Hamburg demonstrates the examination sequence

The EndoRotor® as a completely new mechanical mucosectomy procedure — an alternative for faster ER and ESD?
The EndoRotor® as a completely new mechanical mucosectomy procedure — an alternative for faster ER and ESD?
Stephan Hollerbach and his team demonstrate an en-bloc resection in a swine model using the new mechanical EndoRotor® resection system.

News from DDW
News from DDW
The latest developments in the field of gastroenterology and endoscopy are presented every year at Digestive Diseases Week (DDW) in Chicago — although in recent

Endoscopic Doppler examination and hemostasis in nonvariceal upper gastrointestinal hemorrhage: paradigm shift, or old wine in new bottles?
Endoscopic Doppler examination and hemostasis in nonvariceal upper gastrointestinal hemorrhage: paradigm shift, or old wine in new bottles?
During hemostasis in patients with nonvariceal upper gastrointestinal hemorrhage, the Forrest classification is recommended for risk stratification, as it correlates best with the risk of
Endoscopic diagnosis of celiac disease
Endoscopic diagnosis of celiac disease
Celiac disease is a chronic inflammation trigged by the ingestion of gluten and resulting in a dense infiltration of lymphocytes in the proximal small intestine.

Tunnel removal of a submucosal tumor in the esophagus (SET technique)
Tunnel removal of a submucosal tumor in the esophagus (SET technique)
Dr. Werner and Prof. Rösch from Hamburg present the case of a young patient with an incidental finding of esophageal GIST. In this patient, it

Neuroendocrine Gastric Tumors
Neuroendocrine Gastric Tumors
Among the gastric submucosal tumors, neuroendocrine tumors are a special entity, which also require examination of independent gastric mucosal biopsies for classification.

Heterotopic gastric mucosa
Heterotopic gastric mucosa
Heterotope Magenschleimhaut des Ösophagus (heterotopic gastric mucosa, gastric inlet patch) entspricht funktionellem Magengewebe, das sich nicht an der anatomisch üblichen Lokalisation befindet. Sie ist in

When the Z-line is not completely normal
When the Z-line is not completely normal
Depending on the patient’s degree of sedation and the examiner’s level of experience, carrying out a precise examination of the Z-line may not be very
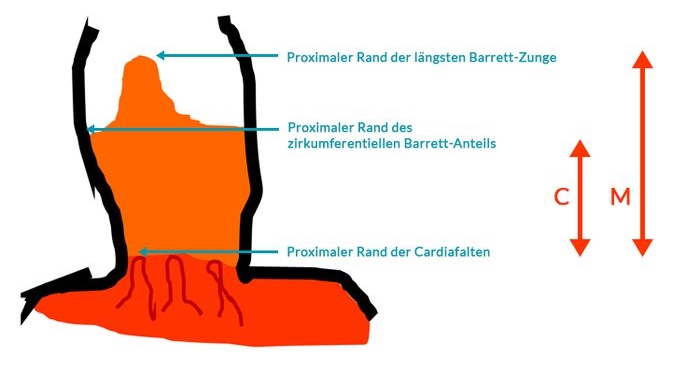
Prague Classification Barrett Esophagus
Prague Classification Barrett Esophagus
The Prague classification was presented by an international research group in 2006 (1) and has since been regarded as the standard for measuring the length

Reflux Esophagitis: Los Angeles Classification
Reflux Esophagitis: Los Angeles Classification
Gastroesophageal reflux disease with endoscopically identifiable lesions (erosions, stricture, Barrett’s esophagus) is defined as erosive gastroesophageal reflux disease (GERD). Fewer than 50% of patients with
Esophageal Varices
Esophageal Varices
Various systems are available for classifying esophageal varices. Unfortunately, they only overlap or coincide partly. The official terminology used by the German Society for Digestive

Endoscopic therapy of pancreatic fluid collections caused by severe necrotic pancreatitis
Endoscopic therapy of pancreatic fluid collections caused by severe necrotic pancreatitis
Pancreatitis can cause various severe complications such as acute fluid collections with superinfected necrotic content requiring drainage and removal of necrotic debris. Here we demonstrate

ESD probably no better than EMR in Barrett’s neoplasia
ESD probably no better than EMR in Barrett’s neoplasia
Considerable debate is currently taking place among therapeutic endoscopists regarding the best method of resecting early carcinomas, particularly in the upper gastrointestinal tract — whereas

Eosinophilic Esophagitis
Eosinophilic Esophagitis
A classification for eosinophilic esophagitis has not yet been included in the usual terminologies in the German-speaking countries. In the official terminology of the German

Post-EMR arterial bleeding
Post-EMR arterial bleeding
Arterial bleeding from the area of the endoscopic mucosal resection, 2 days after the intervention. Successful hemostasis is achieved using bipolar coagulation forceps in “Soft

PEXACT — direct-puncture PEG after gastropexy
PEXACT — direct-puncture PEG after gastropexy
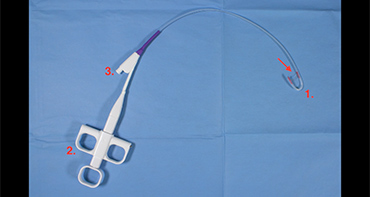
The gastropexy device consists of two hollow needles that are attached to each other. A suture thread is inserted through one hollow needle, and a

Endoscopic division of a Zenker diverticulum using the Clutch Cutter
Endoscopic division of a Zenker diverticulum using the Clutch Cutter
Endoscopic division of a Zenker diverticulum using the Clutch Cutter and management of a perforation. Coagulation of the diverticular septum using the Clutch Cutter. Settings:

Small carcinoma in Barrett’s esophagus — EMR and RFA
Small carcinoma in Barrett’s esophagus — EMR and RFA
A 46-year-old patient with short-segment Barrett’s esophagus that had been receiving monitoring since 2009, now presenting with a mucosal adenocarcinoma.
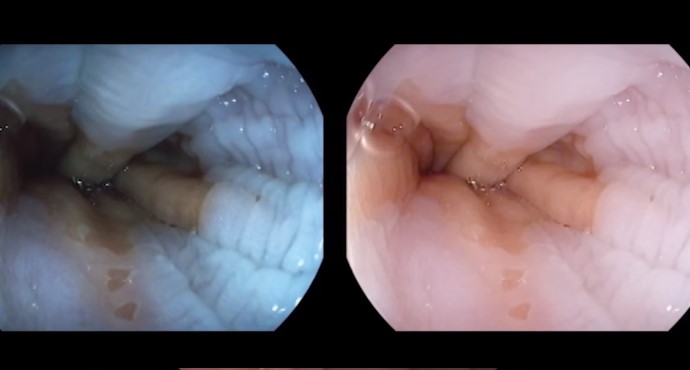
Endoscopic examination of a normal Z-line
Endoscopic examination of a normal Z-line
Visualization of the Z-line without enhancement and with iScan, obstructed by esophageal motility.

Endoscopy antireflux therapy with the MUSE system
Endoscopy antireflux therapy with the MUSE system
A 31-year-old female patient who has had reflux symptoms for 15 years and has responded well to PPI therapy. The patient wants to stop taking

Fundic Varices
Fundic Varices
In contrast to esophageal varices, there is only one classification system for fundic varices, developed by Sarin et al.
Risk stratification in Barrett’s esophagus — the emperor’s new clothes?
Risk stratification in Barrett’s esophagus — the emperor’s new clothes?
The efficacy of surveillance for Barrett’s patients is a matter of controversy, and it is probably due to the low long-term risk of carcinoma developing

Low-grade dysplasia in Barrett’s esophagus — a second opinion is important, but then treatment is needed
Low-grade dysplasia in Barrett’s esophagus — a second opinion is important, but then treatment is needed
Low-grade dysplasia (low-grade intraepithelial neoplasia, LGIN) is difficult to distinguish from inflammation histopathologically. The interobserver variance rates usually show kappa values below 0.4, representing a
Does Barrett’s esophagus grow during monitoring?
Does Barrett’s esophagus grow during monitoring?
The risk of progression of nonneoplastic Barrett’s esophagus to high-grade intraepithelial neoplasia or adenocarcinoma is extremely low and has been reported in recent studies to
Achalasia — place of endoscopic therapy in the light of the first long-term data for POEM
Achalasia — place of endoscopic therapy in the light of the first long-term data for POEM
Achalasia is a rare neuromuscular disease of unclear etiology that probably has a genetic background. The precise etiopathogenesis of achalasia is still unclear. Above all,
