By loading the video, you accept Vimeo's privacy policy.
Learn more
Sequenzen:
 Sequence 1 – Endoscopic and endoscopic ultrasound (EUS) depiction of a submucosal gastric tumor
Sequence 1 – Endoscopic and endoscopic ultrasound (EUS) depiction of a submucosal gastric tumor
A subepithelial tumor has been identified in the fundus. EUS shows that it is 2.5 × 3 cm in size, probably arising from the muscularis propria. No pathological locoregional lymph nodes. No ascites.
 Sequence 2 – Suturing the gastric wall using the GERD-X suturing device
Sequence 2 – Suturing the gastric wall using the GERD-X suturing device
The GERD-X suturing device is introduced into the stomach orally with wire guidance, with the patient deeply sedated but not intubated. A slim-sized endoscope is introduced through the 6-mm working channel in the GERD-X for imaging. Once it has entered the stomach, the device is inverted.
The tissue retractor is then drilled into the gastric wall in the immediate vicinity of the tumor.
A wall duplication is then carried out at the base of the subepithelial tumor, by placing transmural resorbable sutures.
A total of three sutures have been placed, each followed by endoscopic checking of the findings. The sutures are anchored with small PTFE tabs to prevent them from migrating.
 Sequence 3 – Resection of the tumor using a polypectomy snare
Sequence 3 – Resection of the tumor using a polypectomy snare
The full-thickness resection with a monofilament polypectomy snare is now carried out, followed by recovery of the specimen using a Roth net.
Arterial bleeding is controlled using a Coagrasper.
After another inspection, a fourth suture is placed for secure wound closure.
 Sequence 4 – Macroscopic appearance of the specimen after the resection
Sequence 4 – Macroscopic appearance of the specimen after the resection
Macroscopic appearance of the full-thickness resection specimen.
 Sequence 5 – Microscopic appearance of the specimen after resection
Sequence 5 – Microscopic appearance of the specimen after resection
Histologically: full-thickness resection specimen of a gastrointestinal stromal tumor (GIST) (pT2, cM0, N0, L0, V0, R0).
 Sequence 6 – Check-up endoscopy the day after the resection
Sequence 6 – Check-up endoscopy the day after the resection
The check-up examination the following day shows an unremarkable resection site, with extragastric fatty tissue appearing like a “plug.”
Related Posts

Paris classification V
The Paris classification for superficial / early tumors should be
VIEW THE CLASSIFICATION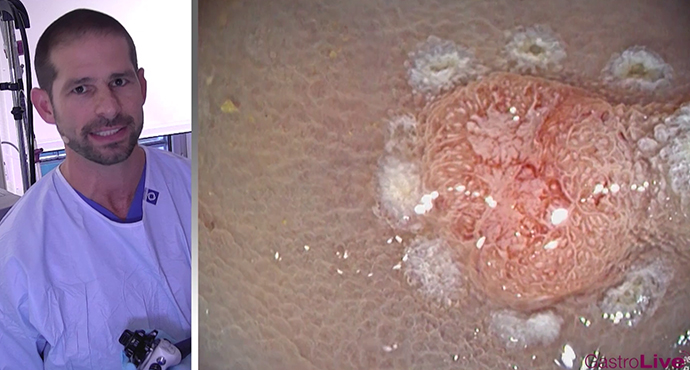
Rectal-Cancer the special case
A 77-year-old patient presented to the emergency department with Hb-relevant
WATCH THE VIDEO