By loading the video, you accept Vimeo's privacy policy.
Learn more
Sequenzen:
 Sequence 1 — resection of the stomach
Sequence 1 — resection of the stomach
This video illustrates the altered anatomy resulting after the type of gastric resection that is carried out for gastric carcinoma, for example. Bowel continuity is reconstructed afterward using a Roux-en-Y loop. The stomach is resected totally or subtotally as far as the duodenal bulb.
 Sequence 2 — reconstructing bowel continuity
Sequence 2 — reconstructing bowel continuity
Continuity is reestablished by pulling up a removed jejunal loop segment. The loop is sutured to the side of the residual stomach, or directly to the esophagus.
The transected duodenal loop is then joined to the jejunal loop laterally or side-to-side.
 Sequence 3 — endoscopic access to the papilla
Sequence 3 — endoscopic access to the papilla
If endoscopy is needed in order to reach the major duodenal papilla, you first pass the anastomosis by moving from the esophagus or residual stomach to the jejunal loop and then reach the jejunojejunostomy further down.
Due to the side-to-side anastomosis, three lumens are seen, one of which ends blindly. The duodenal loop is usually the one that goes off at the least favorable angle.
Accessing the major duodenal papilla after a Roux-en-Y reconstruction is an elaborate procedure that is usually attempted with an enteroscope. Success rates are in the range of 70–80%.
Related Posts
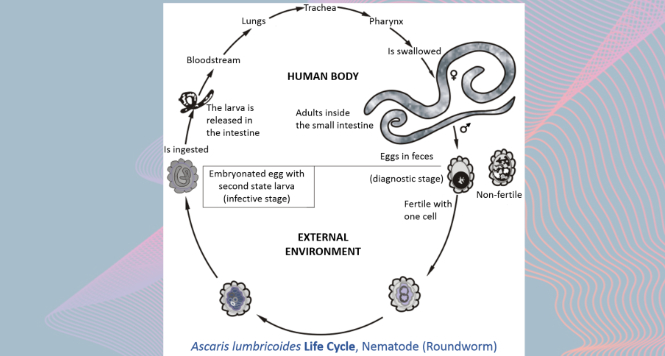
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations
VIEW THE GALLERY
Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal
