Forrest Classification
The Forrest Classification was first described in 1974 by J.A. Forrest et al. in TheLancet1. This classification is a widely used classification of ulcer-related upper gastrointestinal bleeding. It was initially developed to unify the description of ulcer bleeding for better communication amongst endoscopists. However, the Forrest Classification is now used as a tool to identify patients who are at an increased risk for bleeding, rebleeding and mortality2–4.
| Forrest Classification | |
| Acute haemorrhage Forrest Ia Forrest Ib | Active spurter Active oozing |
| Signs of recent haemorrhage Forrest IIa Forrest IIb Forrest IIc | Non-bleeding visible vessel Adherent clot Flat pigmented haematin on ulcer base |
| Lesions without active bleeding Forrest III | Clean-based ulcer |
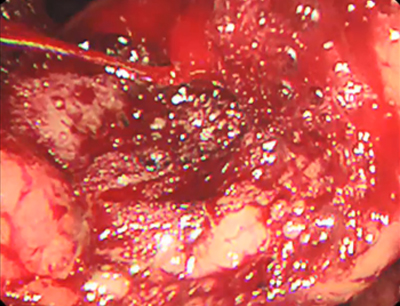
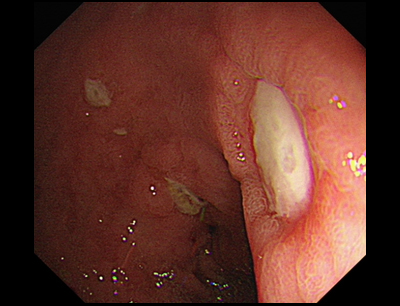
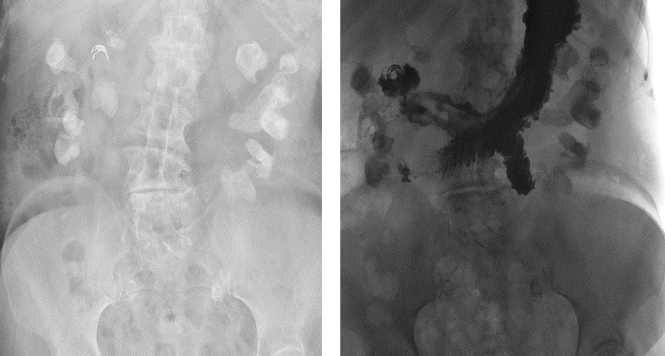
Example illustrations











References:
- Forrest, JA.; Finlayson, ND.; Shearman, DJ. (Aug 1974). ‘Endoscopy in gastrointestinal bleeding’. Lancet. 2 (7877): 394–7.
- Rockall, TA, Logan, RF, Devlin, HB et al. ‘Risk assessment after acute upper gastrointestinal haemorrhage’. Gut 1996; 38: 316–21.
- Guglielmi A, Ruzzenente, A, Sandri, M et al. ‘Risk assessment and prediction of rebleeding in bleeding gastroduodenal ulcer’. Endoscopy 2002; 34: 778–86.
Written by:



Articles
Related Posts


PPI for critically ill ICU patients
PPIs have become routine in ICU units to prevent bleeding in critically ill patients – but …
Our partners:
Publish Your Insights!
Share your papers, videos, articles, or classifi cations on the Endoscopy Campus and reach an international professional audience.
- International Visibility
- Professional Recognition
- Monetary Compensation
- Diverse Contribution Formats
