Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation of the lesion must be accomplished.
White light endoscopy, digital chromo endoscopy and magnification are useful technologies to assess the lesion extension, its limits and the mucosal and microvascular pattern.
Sequenzen:
 Endoscopic evaluation
Endoscopic evaluation
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation of the lesion must be accomplished.
White light endoscopy, digital chromo endoscopy and magnification are useful technologies to assess the lesion extension, its limits and the mucosal and microvascular pattern. In this case, an Olympus 190 series upper GI scope provides narrow band imaging and near focus for a better evaluation.
A sub-cardial 15 mm IIA+IIC early gastric cancer is identified. The preoperative endoscopic biopsy informed a well differentiated adenocarcinoma.
 Marking
Marking
After the lesion limits are clearly identified, marking is made with a ball tip shaped knife applying soft coagulation to the mucosa. It should be performed 2-3 mm away from the lesion to provide a safety margin.
In our institution, we use an ERBE electrosurgical unit for this procedure.
 Submucosal injection
Submucosal injection
An osmotic agent is injected in the submucosal space outside the lesion margins. We prefer using a Voluven based solution with indigo carmine and adrenaline, because it lasts more than saline but is less expensive than sodium hyaluronate.
 Mucotomy
Mucotomy
After completing the submucosal space injection, the needle is exchanged for the ball tip shaped endoscopic knife, which has the ability to cut and also inject the previously described solution as required.
Our group supports a complete circumferential mucotomy before starting the submucosal dissection.
 Submucosal dissection
Submucosal dissection
Submucosal dissection is carried out using the traction provided with the distal attachment. In this particular location, the dissection combines retroflex and forward view scope positions to achieve an en-bloc resection.
Repeated injections of the solution to the submucosal space allows a better visualization of the plane of the dissection, that should be carried out right above the muscular layer.
Small vessels are often encountered during the procedure. Most of them are adequately coagulated with the same knife. Larger ones may require hemostasis with coagulation forceps.
 Specimen extraction and extension
Specimen extraction and extension
Once the dissection is completed, the resected specimen can be retrieved with a Roth net and then extended to allow proper pathological assessment and subsequently determine the curative role of the procedure.
 Ulcer evaluation
Ulcer evaluation
A thorough evaluation of the ulcer is performed to detect muscle layer defects that may require clipping or vessels which should be coagulated.
Patients are kept on high dose intravenous PPIs for the first 24 hours and then maintained orally until endoscopic ulcer healing is certified.
Beiträge
Ähnliche Beiträge
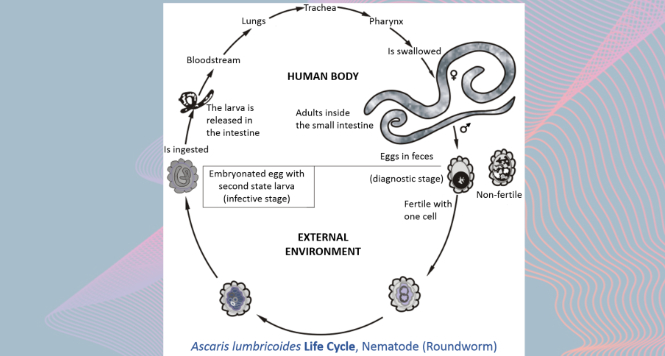
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations as it maybe asymptomatic showing only …
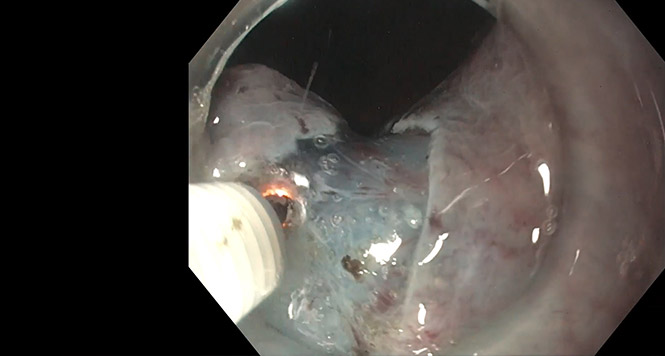
STER for Esophageal Leiomyoma
A two centimeter submucosal lesion arising from muscularis mucosae is identified in the distal esophagus. …
Rectal ESD
In this case, a 65-year-old woman presents with a recurrence of a polyp previously treated with …
