Sub-mucosal Tunneling Endoscopic Resection (STER) of an Esophageal Leiomyoma
A two centimeter submucosal lesion arising from muscularis mucosae is identified in the distal esophagus.
Sequenzen:
 Endoscopic and EUS evaluation
Endoscopic and EUS evaluation
A two centimeter submucosal lesion arising from muscularis mucosae is identified in the distal esophagus.
 Injection
Injection
An osmotic agent, consisting in a Voluven based solution with indigo carmine, is injected in the submucosal space at the level in which the mucotomy is planned.
 Mucotomy
Mucotomy
The needle is exchanged for an endoscopic knife and a longitudinal mucotomy of 15 to 20 mm long is created.
 Submucosal tunneling
Submucosal tunneling
A submucosal tunnel is created from a point 5 cm proximal to the lesion. It is extended the distally until the tumor is identified, using a combination of blunt dissection and coagulation.
Mucosal thermal damage must be prevented so repeated injections in the submucosal space contribute to better exposure.
Small vessels are often encountered in the esophagus submucosal space, that can be sectioned with the same knife. On the other hand, vessels tend to be larger as you approach to the gastric submucosa, that may require the use of coagulation forceps to prevent bleeding.
 Lesion Resection and Extraction
Lesion Resection and Extraction
A pearl-white submucosal tumor is identified during the dissection. The lesion is dissected from the submucosal space and larger feeding vessels are coagulated with coagulation forceps and then sectioned. The distal attachment provides proper traction in order to assist the dissection.
Once the tumor is completely free it is extracted through the mouth by aspirating it into the distal attachment. Larger specimens may require the use of a Roth net.
Finally the specimen is sent to histology assessment. In this case the biopsy informed an esophageal leiomyoma.
 Tunnel Revision
Tunnel Revision
Finally, after assuring adequate hemostasis, a gentamicin based solution is instilled into the tunnel.
 Mucosal Closure
Mucosal Closure
The esophageal mucosa is closed with endoscopic clips starting from the distal end of the defect.
On average five to six clips are used in a standard procedure.
This is a very important step of the procedure, since a clip misplacement may result in esophageal leakage.
Beiträge
Ähnliche Beiträge
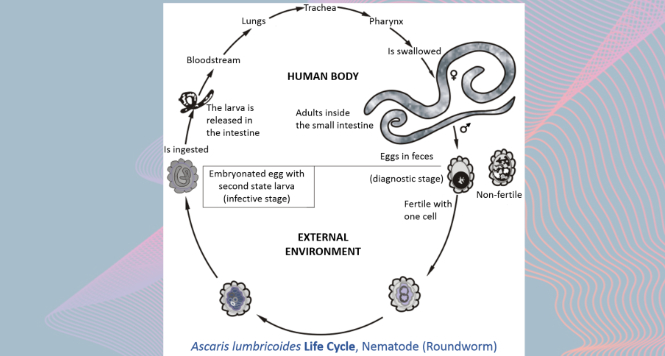
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations as it maybe asymptomatic showing only …

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation …

The black esophagus
A 68-year old woman with advanced endometrial cancer and evidence of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia …
