By loading the video, you accept Vimeo's privacy policy.
Learn more
Sequenzen:
 Endoscopic evaluation
Endoscopic evaluation
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation of the lesion must be accomplished.
 Marking
Marking
After the lesion limits are clearly identified, marking is made with a ball tip shaped knife applying soft coagulation to the mucosa. It should be performed 2-3 mm away from the lesion to provide a safety margin.
 Submucosal injection
Submucosal injection
An osmotic agent is injected in the submucosal space outside the lesion margins. We prefer using a Voluven based solution with indigo carmine and adrenaline, because it lasts more than saline but is less expensive than sodium hyaluronate.
 Mucotomy
Mucotomy
Our group supports a complete circumferential mucotomy before starting the submucosal dissection.
 Submucosal dissection
Submucosal dissection
Submucosal dissection is carried out using the traction provided with the distal attachment. In this particular location, the dissection combines retroflex and forward view scope positions to achieve an en-bloc resection.
 Specimen extraction and extension
Specimen extraction and extension
Once the dissection is completed, the resected specimen can be retrieved with a Roth net and then extended to allow proper pathological assessment and subsequently determine the curative role of the procedure.
 Ulcer evaluation
Ulcer evaluation
A thorough evaluation of the ulcer is performed to detect muscle layer defects that may require clipping or vessels which should be coagulated.
Related Posts
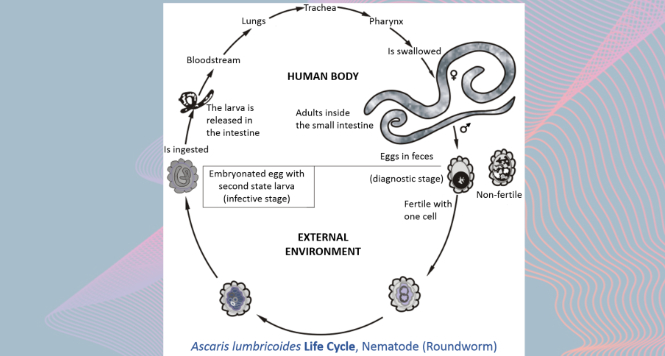
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations
VIEW THE GALLERY
STER for Esophageal Leiomyoma
A two centimeter submucosal lesion arising from muscularis mucosae is
WATCH THE VIDEO