Rectal Endoscopic Submucosal Dissection
In this case, a 65-year-old woman presents with a recurrence of a polyp previously treated with endoscopic mucosal resection. The biopsy and the endoscopic evaluation suggest an adenoma with high grade dysplasia.
Sequenzen:
 Lesion evaluation
Lesion evaluation
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation of the lesion must be accomplished.
White light endoscopy, digital chromo endoscopy and magnification are useful technologies to assess the polyp extension, its mucosal pattern and therefore predict risk of malignancy.
In this case, a 65-year-old woman presents with a recurrence of a polyp previously treated with endoscopic mucosal resection. The biopsy and the endoscopic evaluation suggest an adenoma with high grade dysplasia.
 Submucosal injection
Submucosal injection
An osmotic agent is injected in the submucosal space outside the lesion margins. We prefer using a Voluven® based solution with indigo carmine and adrenaline, because it lasts more than saline but is less expensive than sodium hyaluronate.
 Mucotomy
Mucotomy
After completing the submucosal space injection, the needle is exchanged for an endoscopic knife. In this case we used a ball tip shaped one with the ability to inject the previously described solution.
Traditionally in esophageal and gastric endoscopic submucosal dissection marking outside the lesion limits is required before the mucotomy. Nevertheless, in colonic and rectal lesions this is not necessary.
As you may recognize in this video, the margins of the polyp are clearly identified after the submucosal space injection.
Our group supports a complete circumferential mucotomy before starting the submucosal dissection.
 Submucosal dissection
Submucosal dissection
Submucosal dissection is carried out using the traction provided with the distal attachment.
Repeated injections of the solution to the submucosal space allows a better visualization of the plane of the dissection, that should be carried out right above the muscular layer.
Small vessels are often encountered during the procedure. Most of them are adequately coagulated with the same knife. Larger ones may require hemostasis with coagulation forceps.
Once the dissection is completed, the resected specimen can be retrieved with a Roth net.
 Rectal ulcer evaluation
Rectal ulcer evaluation
A thorough evaluation of the ulcer is performed to detect muscle layer defects that may require clipping or vessels which should be coagulated.
 Specimen extension
Specimen extension
Tissue extension of the lesion prevents shrinking and allows a proper pathological assessment in order to evaluate margins and subsequently determine the curative role of the procedure.
Beiträge
Ähnliche Beiträge
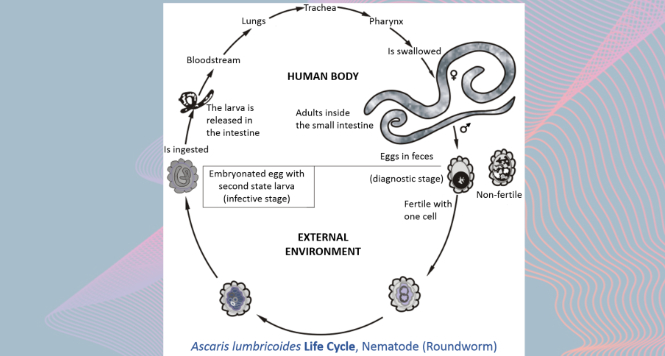
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations as it maybe asymptomatic showing only …

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation …
STER for Esophageal Leiomyoma
A two centimeter submucosal lesion arising from muscularis mucosae is identified in the distal esophagus. …
