Endoscopic therapy in sigmoid volvulus — case report and glance at the current ASGE guideline
Clinical case: A 78-year-old lady presented as an emergency case with stool retention for several days in chronic constipation, with known diverticulosis and acutely increasing abdominal pain. She was bedridden due to syringomyelia. An emergency CT provided findings of colonic ileus with suspected sigmoid volvulus.
Glance at the guideline: Along with the cecum, the sigmoid colon is the most frequent site of manifestation for intestinal volvulus. Rotation occurs along the mesenterial axis of the mobile sigmoid. The patients present with colonic obstruction that may continue as far as the clinical picture of ileus. Sigmoid volvulus more often affects men over the age of 70, diabetic patients, those with prior abdominal surgery, those with a tendency to develop constipation, and patients with prior neuropsychiatric conditions. By contrast, volvulus in the cecum more often affects young women.
Once the diagnosis has been confirmed using computed tomography (showing the “coffee bean sign”), sigmoidoscopic detorsion is recommended as the primary therapy if there is no peritonitis, perforation, or the course is not recurrent [1]. In cecal volvulus, by contrast, surgical therapy is preferred due to lower success rates and higher perforation rates.
Sigmoidoscopy shows a spiral stenosis in the colon mucosa. It is recommended to advance past this while observing the greatest possible caution and then to decompress aggressively. Placement of a decompression probe may then be considered. The primary success rate with endoscopy ranges from 55% to 94% [1]. As there is a substantial rate of recurrence after endoscopic detorsion, the ASGE Guideline recommends elective sigmoid resection in operable patients [1].
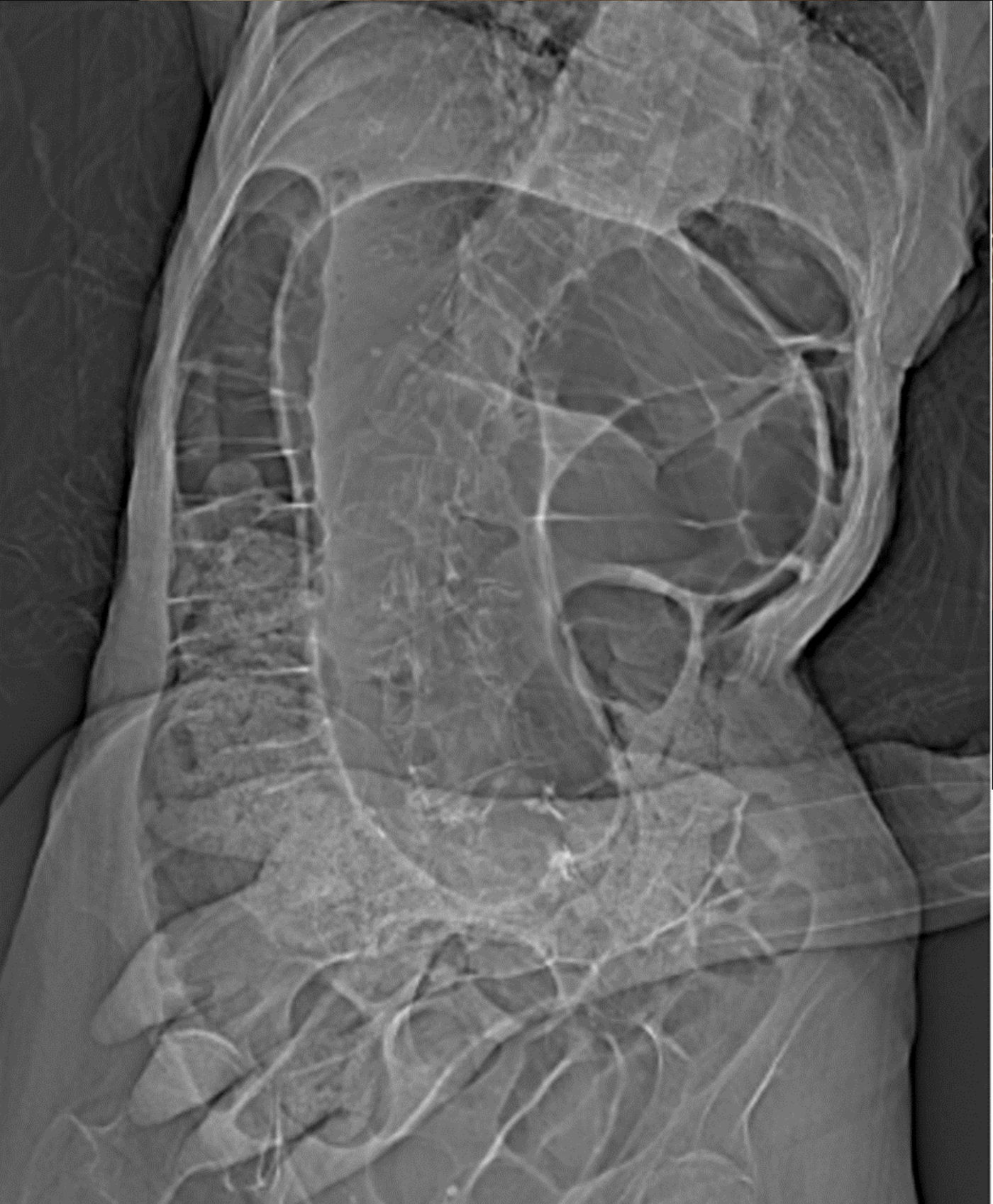
Fig. 1: Abdominal CT topogram showing the typical “coffee bean sign” in sigmoid volvulus. 
Fig. 2: A typical spiral stenosis is seen at the rectosigmoid junction during endoscopic decompression. 
Fig. 3: Rapid decompression proximal to the stenosis in the sigmoid. The colon mucosa shows marked hypervolemia. 
Fig. 4: Check-up sigmoidoscopy 2 days after detorsion, showing superficial ischemic mucosal necrosis with a sharp demarcation in the area of the rectosigmoid junction. 
Fig. 5: Check-up sigmoidoscopy: the venous congestion in the sigmoid has resolved. Superficial mucosal alteration is present — with an appearance as in ischemic colitis.
Reference:
- Mariam Naveed, Laith H. Jamil, Larissa L. Fujii-Lau, Mohammad Al-Haddad, James L. Buxbaum, Douglas S. Fishman, et al. American Society for Gastrointestinal Endoscopy guideline on the role of endoscopy in the management of acute colonic pseudo-obstruction and colonic volvulus Gastrointest Endosc February 2020, Volume 91, Issue 2, Pages 213-227.e6 / DOI: https://doi.org/10.1016/j.gie.2019.04.231
Our partners:
Publish Your Insights!
Share your papers, videos, articles, or classifi cations on the Endoscopy Campus and reach an international professional audience.
- International Visibility
- Professional Recognition
- Monetary Compensation
- Diverse Contribution Formats
