The EndoRotor® as a completely new mechanical mucosectomy procedure — an alternative for faster ER and ESD?
Stephan Hollerbach and his team demonstrate an en-bloc resection in a swine model using the new mechanical EndoRotor® resection system.
Sequenzen:
 Sequence 1 — marking an esophageal lesion
Sequence 1 — marking an esophageal lesion
The video initially shows the site after submucosal injection of a mucosal lesion in the distal esophagus. The lesion had been previously identified and marked.
 Sequence 2 — incision from the oral margin
Sequence 2 — incision from the oral margin
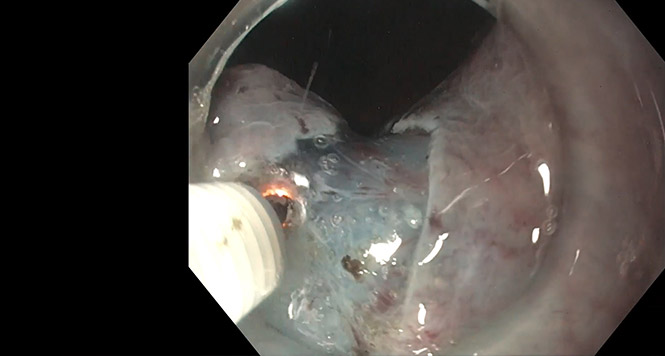
Using the mechanical rotating EndoRotor® catheter head, a proximal incision is then made into the submucosa on the margin of the lesion. In the process, the catheter sucks the mucosal segment involved into an opening in which two small rotating knives resect the mucosal segment and deposit all of the resected matter into a filter, so that all of the tissue particles can be examined histologically afterwards — including the margins.
 Sequence 3 — submucosal tunneling of the lesion
Sequence 3 — submucosal tunneling of the lesion
After the incision, the catheter is now advanced carefully into the submucosa, which is mechanically separated so that a “tunnel” is created. The endoscope is then introduced into the tunnel from proximal to distal, and a large submucosal space is bluntly dissected using the endoscope and the mechanical catheter. N.B.: this technique does not require any use of a knife, any thermal cutting, or any electric current.
 Sequence 4 — dissection of the aboral margin and sides
Sequence 4 — dissection of the aboral margin and sides
After the overlying mucosal area has been lifted for endoscopic submucosal dissection (ESD), the distal end and the two lateral edges are incised using suction and mechanical cutting, until finally the resection specimen is released.
The specimen is then withdrawn “en bloc” using forceps.
 Sequence 5 — ablation surface and histological examination
Sequence 5 — ablation surface and histological examination
Inspection of the ablation area shows that deep ablation has been achieved as far as the last third of the submucosa, above the muscularis layer in the esophagus. Histopathological examination of the removed esophagus (post mortem) shows resection as far as the lowest layer of the submucosa. No relevant bleeding or perforations occurred in any of n = 4 repeated esophageal resections.
Articles
Related Posts

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation …
Rectal ESD
In this case, a 65-year-old woman presents with a recurrence of a polyp previously treated with …

ESD Esophagus
Early esophageal carcinoma (squamous epithelium): tips and tricks for difficult ESDs …
