Refractory Gastroparesis: Expert Recommendations
Vanessa M. Shami, MD, FASGE, reviewing Lacy BE, et al. Clin Gastroenterol Hepatol 2021 Oct 29.
Gastroparesis is a vexing problem and often has overlapping symptoms with functional dyspepsia. In this update from the American Gastroenterological Association, medically refractory gastroparesis is defined as ongoing symptoms in patients with a confirmed diagnosis of gastroparesis despite appropriate dietary changes and the use of metoclopramide as a first-line therapeutic agent. Algorithms for the diagnosis and management of refractory gastroparesis have not been standardized due to a lack of prospective studies to determine the best approach for these patients. The authors of this clinical practice update used published data and expert review to outline a strategy to define, diagnose, and manage refractory gastroparesis.
Best practice advice:
- Exclude disorders that can be confused for medically refractory gastroparesis, including mechanical obstruction, hypothyroidism, adrenal insufficiency, and functional dyspepsia.
- Confirm that the diagnosis is made when the patient is no longer using opioids to manage pain and when the appropriate 4-hour gastric emptying test is employed.
- Classify patients with gastroparesis based on symptoms and results of a gastric emptying study: mild (10%-15% retention at 4 hours), moderate (15%-35%), or severe (>35%).
- Identify the predominant symptom (nausea and/or vomiting vs abdominal pain and/or discomfort), and initiate treatment accordingly.
- Antiemetics and prokinetics are options for treating nausea and vomiting.
- Neuromodulators should be tried for patients with abdominal pain, whereas opioids should be avoided.
- Consider gastric electrical stimulation in patients with refractory nausea and vomiting who have failed other therapies; it is not recommended in patients with pain-predominant gastroparesis.
- Consider gastric peroral endoscopic myotomy in a multidisciplinary center for patients with gastroparesis who have severely delayed gastric emptying.

COMMENTThe key to the diagnosis of gastroparesis is to, first, exclude mimicking etiologies and diagnose with the appropriate tests. Once diagnosed, the predominant symptom should be identified, and patients should be treated accordingly for nausea and/or vomiting versus abdominal pain.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Lacy BE, Tack J, Gyawali CP. AGA Clinical Practice Update on management of medically refractory gastroparesis: expert review. Clin Gastroenterol Hepatol 2021 Oct 29. (Epub ahead of print) (https://doi.org/10.1016/j.cgh.2021.10.038)
Beiträge
Ähnliche Beiträge
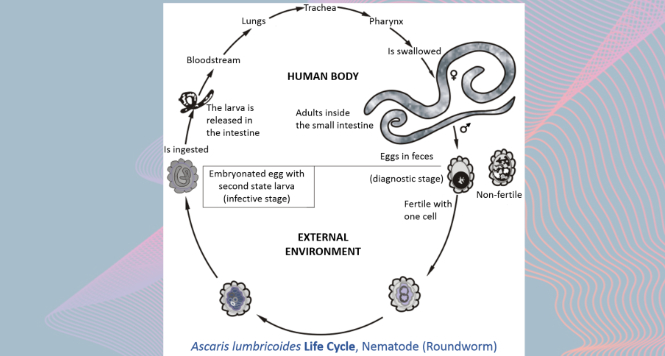
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations as it maybe asymptomatic showing only …

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation …
