Refractory Celiac Disease: What to Do
Vanessa M. Shami, MD, FASGE, reviewing Green PHR, et al. Gastroenterology 2022 Sep 19.
Refractory celiac disease (RCD) is defined as celiac disease with persistent symptoms despite at least 12 months of a strict gluten-free diet. There are 2 subtypes of RCD: type 1 is similar to the conventional disease, with villous atrophy and intraepithelial lymphocytes, whereas type 2 is unique because it has the potential for aberrant clonal T-cell expansion in the GI tract and other organs, increasing the likelihood of ulcerative jejunoileitis or enteropathy-associated T-cell lymphoma. This second subtype carries an overall poorer diagnosis.
This practice update from the American Gastroenterological Association, developed with evidence from published data and expert review, provides best practice advice for the diagnosis and management of RCD.
Best practice advice:
- In patients with persistent symptoms despite treatment, the initial diagnosis of celiac disease should be confirmed by a review of prior testing.
- In patients with persistent symptoms despite treatment, ongoing gluten ingestion should be excluded. EGD with small bowel biopsies should be performed to look for villous atrophy. If villous atrophy persists or the initial diagnosis of celiac disease was not confirmed, other causes of villous atrophy should be considered.
- If ongoing gluten ingestion is excluded, other potential causes of symptoms, including functional bowel disorders, microscopic colitis, pancreatic insufficiency, inflammatory bowel disease, lactose or fructose intolerance, and small intestinal bacterial overgrowth, should be excluded.
- Flow cytometry, immunohistochemistry, and T-cell receptor rearrangement studies should be used to distinguish between RCD subtypes and exclude enteropathy-associated T-cell lymphoma.
- If subtype 2 RCD is diagnosed, small bowel imaging with capsule endoscopy and computed tomography or magnetic resonance enterography should be performed to exclude enteropathy-associated T-cell lymphoma and ulcerative jejunoileitis.
- A detailed nutritional assessment that includes an investigation of micronutrient and macronutrient deficiencies should be performed in all patients with RCD.
- All macronutrient and micronutrient deficiencies should be corrected. Parenteral nutrition support may be necessary for patients with severe malnutrition due to malabsorption.
- First-line therapy in patients with RCD is open-capsule budesonide or, if unavailable, prednisone.
- Patients with RCD need to be followed by a multidisciplinary team to assess clinical and histologic responses to therapy.
- If patients do not respond to steroids, referral to a center that specializes in RCD is recommended.

COMMENTRCD is a vexing problem for patients and their health care providers. If symptoms persist despite treatment, confirming the diagnosis and ruling out ongoing gluten exposure is essential. Steroids are the first-line treatment for patients diagnosed with RCD.
Note to readers: At the time we reviewed this paper, its publisher noted that it was not in final form and that subsequent changes might be made.
CITATION(S)
Green PHR, Paski S, Ko CW, Rubio-Tapia A. AGA clinical practice update on management of refractory celiac disease: expert review. Gastroenterology 2022 Sep 19. (Epub ahead of print) (https://doi.org/10.1053/j.gastro.2022.07.086)
Beiträge
Ähnliche Beiträge
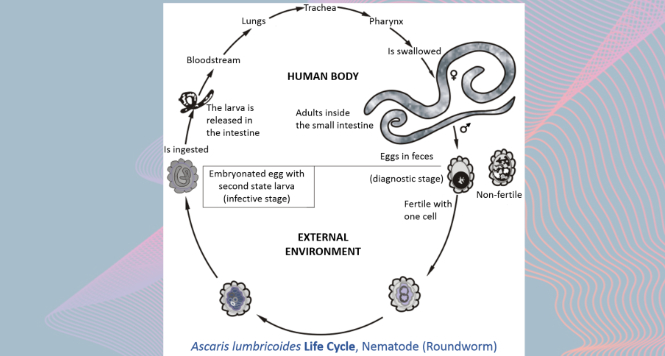
Gastric Ascaris Lumbricoides
Ascaris infestation show quite a wide array of clinical manifestations as it maybe asymptomatic showing only …

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal dissection, a proper and extensive evaluation …
