By loading the video, you accept YouTube's privacy policy.
Learn more
Sequenzen:

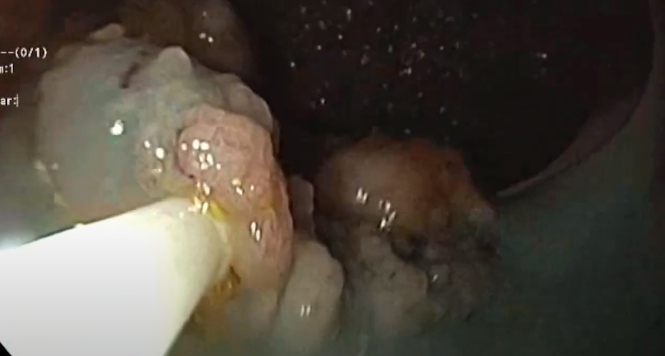
In this 71-year-old patient in whom a squamous-cell carcinoma had been diagnosed at an outside institution, areas of reddish discoloration with whitish surface spots stand out more clearly from their surroundings on narrow-band imaging. The surface is also bumpy and irregular. Before endoscopic submucosal dissection (ESD), marks are placed outside the lesion, at a distance of at least 3–4 mm from the visible margin of the tumor.

After the first incision using the “dual knife,” submucosal connective tissue that is rich in blood vessels appears. Dissection is carried out using the extensible and retractable knife, with cutting current or mixed current, or with coagulation current for the vessels. When dissection is complete, the entire lesion with the incision around it is visible.

During subsequent dissection, the highly vascularized connective tissue under the tumor is mainly dissected with various types of coagulation current (e.g., Swift Coag). The tissue is spread apart using the cap. Repeated spraying is carried out, in this case with slightly viscous Gelafundin.

After the tissue has been spread apart with the cap, it is separated layer by layer and small vessels are obliterated. Repeated spraying is necessary.

What is known as the insulated-tip (IT) knife is used here. With its porcelain insulation, it protects the muscularis layer. The knife is attached laterally and can then be drawn upwards along with the device, even without direct visualization.

The final steps of the dissection on the lower margin are also carried out with the IT knife. On the inhomogeneous resection surface, residual vessels and small superficial muscle defects are closed with clips. The mounted specimen, with its margins macroscopically tumor-free, is inspected. Histological analysis showed sm1 infiltration.
Related Posts

Sub-cardial Gastric ESD
Before starting any endoscopical procedure, in particular an endoscopic submucosal
Piecemeal EMR rectum
Piecemeal endoscopic mucosal resection (EMR) of an extensive laterally spreading
WATCH THE VIDEO