Tokyo Classification Cholangitis (Guidelines)
P. Sauer, Heidelberg
Acute cholangitis results from disturbed biliary drainage and bacterial infection. The mortality rates due to acute cholangitis reported in the literature over the last 20 years are in the range of 3–10%, and, despite the improvement in the prognosis in comparison with earlier studies, mortality continues to be a feared complication of biliary obstruction. The most frequent cause of the drainage disorder is choledocholithiasis, followed by malignant and benign stenoses [1]. Endoscopic treatment for the biliary obstruction as quickly as possible and immediate antibiotic treatment significantly reduce the mortality rate [2].
The clinical presentation of acute cholangitis is not always clear. The Charcot triad typically described in the standard works on the topic has been observed in only 16% to a maximum of 72% of cases in various studies [3].
The diagnostic criteria set out in the updated 2018 Tokyo Guidelines (Table 1) allow a high degree of diagnostic accuracy in routine clinical work, provide reproducible parameters for clinical studies, and have in the meantime been included in other recommendations and guidelines [4].
Table 1 Criteria for acute cholangitis
| A Systemic inflammation | |
| Fever (> 38 °C) or shivering | |
| Laboratory chemistry pattern of inflammation (leukocytes < 4,000 or > 10,000/µL; CRP > 1 mg/dL) |
|
| B Cholestasis | |
| Icterus (bilirubin > 2 mg/dL) | |
| Raised cholestasis parameters and transaminases (ALP, GGT, AST, ALT [IU] > 1.5 times upper limit) |
|
| C Imaging (initially transabdominal ultrasound, followed by endoscopic ultrasound or MRCP) | |
| Bile duct dilation > 7 mm | |
| Evidence of stone or obstruction | |
In the presence of pathological findings, all three diagnostic criteria (A + B + C) can be regarded as definitely confirming obstructive cholangitis. If one pathological finding from category A and another from categories B or C are present, then at least an urgent suspicion of obstructive cholangitis can be noted.
The severity of acute cholangitis is also defined in the Tokyo Guidelines (Table 2). This is decisive in determining the necessity and timing of early intervention for biliary drainage, as well as the indication for intensive-care measures [5]. The current Level 3 guideline on the diagnosis and treatment of cholecystolithiasis in Germany [4] consequently also recommends intervention with stone extraction or drainage as quickly as possible in patients with obstructive stone-related acute cholangitis and also in biliary pancreatitis with cholestasis/icterus and/or cholangitis. In patients with severe cholangitis (grade III), immediate drainage or removal of the obstruction is required. It is important to assess the severity of the cholangitis, not only at first contact with the patient, but also during the subsequent course, since a deteriorating severity grade with an unfavorable prognosis may develop, particularly when there is insufficient biliary drainage.
Table 2 Grades of severity in acute cholangitis
| Mild acute cholangitis | |
| Cholangitis with no criteria for grade II or III acute cholangitis | |
| II Moderately severe acute cholangitis | |
| Cholangitis with evidence of at least two of the following criteria | |
| Leukocytosis > 12,000/µL or leukopenia < 4,000/µL | |
| Fever > 39 °C | |
| Age > 75 years | |
| Bilirubin > 5 mg/dL | |
| Albumin < 25 g/L | |
| III Severe acute cholangitis | |
| Cholangitis with dysfunction of one of the following organs / organ systems | |
| Shock requiring catecholamines | |
| Clouding of consciousness | |
| Pulmonary failure | |
| Renal failure | |
| Hepatic failure | |
| Failure of coagulation | |
References
- Kimura Y, Takada T, Strasberg SM, et al. TG13 current terminology, etiology, and epidemiology of acute cholangitis and cholecystitis. J Hepatobiliary Pancreat Sci. 2013; 20: 8-23.
- Ayub K, Imada R, Slavin J. Endoscopic retrograde cholangiopancreatography in gallstone-associated acute pancreatitis. Cochrane Database Syst Rev. 2004: CD003630. Update in: Cochrane Database Syst Rev. 2010:CD003630.
- Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018; 25: 41-54.
- Gutt C, Jenssen C, Barreiros AP, et al. Updated S3-Guideline for Prophylaxis, Diagnosis and Treatment of Gallstones. German Society for Digestive and Metabolic Diseases (DGVS) and German Society for Surgery of the Alimentary Tract (DGAV) – AWMF Registry 021/008. Z Gastroenterol. 2018; 56: 912-966.
- Miura F, Okamoto K, Takada T, et al. Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis. J Hepatobiliary Pancreat Sci. 2018; 25: 31-40.
Related Posts
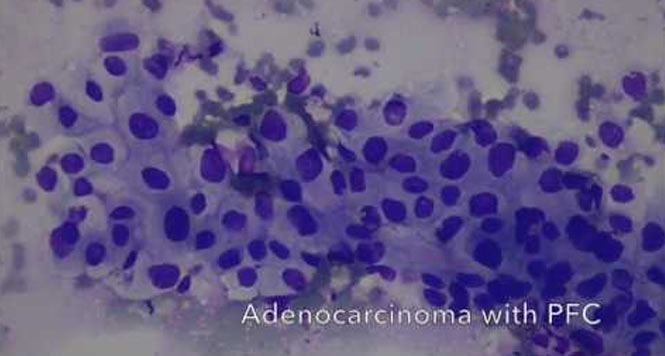
Cancer within a Pancreatic Fluid Collection
This video demonstrates EUS-guided drainage of a pancreatic fluid collection,
WATCH THE VIDEO
Challenges of EUS-FNA
This video demonstrates the challenges associated with EUS-guided FNA of
WATCH THE VIDEO